
Injection for Sciatica in Singapore: Types, How They Work, and When You Need One
June 9, 2026
CONTENTS
- Why an Injection Works Differently From Tablets?
- When Should You Consider an Injection for Sciatica?
- Types of Injection for Sciatica Available in Singapore
- How the Right Injection Is Chosen: The Painostic® Approach
- Situations Where an Injection Alone Is Not Enough
- What to Expect From an Injection Appointment
- When Should You See a Specialist?
- Conclusion
Quick Answer:
An injection for sciatica is appropriate when rest, physiotherapy, and oral medication have not brought enough relief after four to six weeks, when leg pain is severe enough to affect sleep or daily function, or when nerve weakness is present. Several options are available in Singapore: epidural analgesia targets inflamed nerve roots in the spine, peripheral nerve blocks target a single nerve, Coreflex Injections address muscular compression, and pulsed radiofrequency desensitises a chronically irritated nerve. The right choice depends on a confirmed diagnosis of the nerve source, not on symptom severity alone.
Sciatica is not just back pain. It is the sharp, burning, electric sensation that shoots from the lower back through the buttock and down the leg, sometimes reaching the calf or foot. For many patients, the pain is manageable at first. They try rest, over-the-counter anti-inflammatories, and a course of physiotherapy. For some, that is enough.
But for a significant number of patients in Singapore, conservative measures provide only partial relief, or the pain returns within weeks. This is where an injection for sciatica becomes relevant. Not as a last resort, and not as a replacement for diagnosis, but as a targeted intervention that reaches the nerve inflammation that oral medication cannot.
This article focuses on the injection options available for sciatica in Singapore: what each one does, how it is delivered, which clinical situations each suits best, and how to know when an injection is the appropriate next step.
Why an Injection Works Differently From Tablets?
When you take an oral anti-inflammatory, the medication travels through the bloodstream and spreads throughout the body. Only a small fraction reaches the inflamed nerve root in the lumbar spine. By the time it gets there, the concentration is often too low to fully calm the localised swelling pressing on the nerve.
An injection for sciatica changes this entirely. The medication is delivered directly to the site of inflammation, right at the compressed nerve root or the irritated nerve pathway. The concentration at the target is far higher, the onset of relief is faster, and the effects last longer because the drug is not diluted across the whole body.
This is why injections are not simply a stronger version of painkillers. They are a different delivery method that reaches a level of treatment oral medication cannot match.
According to a study published in the Singapore Medical Journal, up to 80% of Singaporeans will experience lower back pain at some point in their lives. Sciatica, arising from a compressed lumbar nerve root, is one of the most common and disabling forms of that pain. For patients in whom conservative care is insufficient, a targeted injection remains the most clinically validated non-surgical option.
When Should You Consider an Injection for Sciatica?
This is the question most patients in Singapore ask when they walk into a pain clinic. There is no single trigger point, but there are clear clinical situations where an injection becomes the right next step. The decision should always follow a proper diagnosis confirming which nerve is compressed and why.
When Conservative Care Has Not Been Enough
The standard first approach for sciatica is activity modification, physiotherapy, and oral medication. For many patients, a course of anti-inflammatories combined with targeted physiotherapy over four to six weeks produces meaningful improvement. If that has happened, there is no reason to proceed to injection.
If, however, you have completed four to six weeks of consistent conservative treatment and the leg pain remains significant, an injection is a reasonable next step. Significant here means pain that limits your daily activities, disrupts your sleep, or prevents you from doing physiotherapy exercises properly. The injection does not replace physiotherapy. In many cases, it makes physiotherapy possible again by reducing pain enough for movement.
When the Pain Is Severe From the Start
Not every patient should wait six weeks before considering an injection. When sciatica is severe from the outset, with leg pain rated seven or above on a ten-point scale, or pain that makes it impossible to sit, stand, or sleep, an earlier injection is clinically appropriate.
Severe acute sciatica from a significant disc herniation carries a risk of prolonged nerve compression if left unmanaged. Getting the inflammation under control quickly can shorten recovery and reduce the risk of lasting nerve damage.
When Nerve Weakness or Numbness Is Present
Sciatica with leg weakness, foot drop, or patches of numbness is a sign of significant nerve root involvement. Waiting several weeks for conservative care to work may not be appropriate in these cases. The nerve needs the compression and inflammation addressed promptly to give it the best chance of full recovery.
If one leg feels weaker than the other on stairs, your foot drags slightly when walking, or a patch of skin on your leg or foot has lost sensation, these are signs that prompt specialist assessment and an early injection for sciatica should be considered.
When Pain Keeps Returning Despite Rest
Some patients experience a cycle of sciatica flares. The pain settles with rest, then returns within days or weeks of resuming normal activity. This pattern suggests the underlying nerve compression has not resolved. An injection can break this cycle by addressing the residual inflammation and reducing nerve sensitivity, giving the spine a proper window to recover.
When Surgery Has Been Recommended and You Want Alternatives First
A number of patients in Singapore are referred to a pain specialist after being told surgery may be needed. In many cases, a carefully chosen injection-based plan, guided by an accurate Painostic® diagnosis, can achieve sufficient relief to avoid or defer surgery. This is not always possible, but it is often worth exploring before committing to an operation.
When You Are Not Yet a Candidate for Surgery
Some patients have conditions that make surgery higher risk, such as anticoagulant use, uncontrolled diabetes, or significant cardiovascular disease. For these patients, minimally invasive injection-based procedures are often the most appropriate route to sustained pain relief.
Types of Injection for Sciatica Available in Singapore
Each injection type targets the nerve differently. Choosing the right one depends on where the nerve is compressed, what is causing that compression, and what a thorough diagnostic assessment confirms.
Epidural Analgesia
Epidural Analgesia is the most widely used injection for sciatica from lumbar disc herniation or spinal stenosis. The procedure delivers a combination of corticosteroid and local anaesthetic into the epidural space, which is the area surrounding the nerve roots as they exit the spinal cord. The corticosteroid reduces inflammation of the compressed nerve root. The local anaesthetic calms the pain signals being transmitted along it.
The most precise approach is a transforaminal epidural injection, where the needle is guided to the specific opening in the spine through which the affected nerve exits. This targets the inflamed nerve root directly, rather than flooding the broader epidural space. Image guidance is used throughout to ensure accurate placement.
A systematic review in the journal Spine found that epidural steroid injections provide meaningful short-to-medium-term pain relief for sciatica caused by disc herniation, with the strongest effect in the first three months. Epidural Analgesia is best suited to patients with confirmed disc herniation or moderate spinal stenosis where the nerve root is inflamed but not yet severely compressed.
[→ Learn more about Spinal Stenosis | Slipped Disc]
Peripheral Nerve Block
A Peripheral Nerve Block involves injecting local anaesthetic and anti-inflammatory medication around a specific nerve or nerve bundle, rather than into the epidural space. For sciatica, this may mean targeting a specific lumbar nerve root at its exit point, or targeting the sciatic nerve in the buttock.
The Peripheral Nerve Block has a dual function that makes it valuable in the diagnostic process. When used to block a single suspected nerve root, the degree of relief it produces confirms whether that nerve is the source of the sciatica. If the block resolves the leg pain, the diagnostic question is answered. If it gives only partial relief, another nerve or structure is also contributing.
For sciatica from piriformis syndrome, where the sciatic nerve is compressed by the piriformis muscle in the buttock rather than by a spinal problem, the Peripheral Nerve Block is the preferred treatment. An epidural in this situation treats the wrong location. The block can be placed directly at the site of nerve irritation in the buttock, providing targeted relief where it is actually needed.
[→ Learn more about Piriformis Syndrome]
Coreflex Injections
Coreflex Injections use a combination of local anaesthetic, anti-inflammatory medication, and muscle relaxant, delivered to the specific tissue causing nerve irritation. For sciatica with a muscular component, including cases where tight muscles around the lumbar spine or piriformis are contributing to nerve compression, Coreflex Injections break the pain-spasm cycle, reduce local inflammation, and restore movement.
They are particularly appropriate for patients whose sciatica has a significant muscular driver alongside the nerve irritation. Coreflex Injections are a well-tolerated first-line interventional option and can often be given in an outpatient setting without the preparation required for epidural procedures.
Pulsed Radiofrequency (PRF)
Pulsed Radiofrequency is a procedure that uses radiofrequency energy delivered in short pulses to desensitise a pain-generating nerve. Unlike conventional radiofrequency ablation, PRF does not destroy the nerve. It applies low-temperature energy in a pulsed pattern that disrupts the nerve’s ability to send pain signals while preserving normal sensory and motor function.
PRF is most appropriate for chronic or recurrent sciatica where the nerve itself has become sensitised. This means the nerve continues to fire pain signals even after the original compression has partially resolved. This pattern is called central sensitisation. These patients often describe persistent burning or electrical pain in the leg that no longer responds to further epidural injections, because the problem is now in the nerve’s firing pattern rather than in the surrounding inflammation.
PRF can be applied to the dorsal root ganglion, which is a cluster of nerve cells along the path of the affected spinal nerve root. This targeted approach has shown good results for chronic neuropathic sciatica in clinical studies.
Nucleoplasty
Nucleoplasty is a minimally invasive procedure for sciatica caused by a herniated disc. It is performed using a fine needle inserted into the disc and done as an outpatient procedure without open surgery. Controlled plasma energy removes a small amount of disc material from within, reducing internal disc pressure and allowing the herniated portion to retract away from the nerve root.
Nucleoplasty suits patients with early to moderate disc herniation who have not achieved enough relief from epidural injections alone. It addresses the mechanical source of nerve compression, not just the inflammatory response to it. The procedure is performed under image guidance and typically takes under an hour. Most patients return to light activity within a few days.
[→ Learn more about Slipped Disc]
Radiofrequency Ablation (RFA)
Radiofrequency Ablation is used when sciatica has a significant facet joint component. In some patients, degenerative changes in the lumbar facet joints produce both local back pain and referred leg pain that mimics sciatica. In others, facet joint inflammation narrows the space around the nerve exit and makes existing sciatica worse.
RFA uses radiofrequency energy to heat and disrupt the medial branch nerves that carry pain signals from the facet joints. Relief typically lasts from six months to over a year. RFA is not a first-line injection for sciatica but is considered when a diagnostic medial branch block has confirmed that the facet joints are a meaningful contributor to the patient’s pain.
How the Right Injection Is Chosen: The Painostic® Approach
At Singapore Paincare, the selection of an injection for sciatica is guided by the Painostic® methodology, a four-pillar diagnostic framework developed by Dr. Bernard Lee Mun Kam. It evaluates pain patterns, underlying pathology, how the nervous system is processing the pain, and any psychological factors influencing the patient’s experience of pain.
This process involves a detailed pain history, physical examination of nerve tension signs and leg strength, MRI or CT imaging to identify the structural cause, and where needed, a diagnostic nerve block to confirm the target level. The result is a personalised Injection Roadmap that sequences the most appropriate procedures in the least invasive order.
Choosing the wrong injection, or performing it at the wrong spinal level, is one of the most common reasons patients feel that injections did not work. The procedure is sound. The target was simply incorrect. A thorough Painostic® assessment is designed to prevent this.
For a full overview of how sciatica is managed from first presentation to treatment, visit the Singapore Paincare sciatica treatment page. For patients with concurrent back pain or slipped disc involvement, the back pain specialist page covers how spinal assessments are conducted.
Situations Where an Injection Alone Is Not Enough
It is equally important to be clear about when an injection for sciatica is not the complete answer on its own.
If the structural cause of sciatica has not been addressed, such as a large disc herniation or severe spinal stenosis, injections can provide relief but the pain may return when the effect wears off. In these cases, the injection buys time and reduces inflammation while the structural issue is assessed for more definitive treatment such as nucleoplasty or endoscopic laser decompression.
An injection cannot treat sciatica caused by active infection, spinal tumour, or fracture. These require specific medical or surgical management and should be identified during the diagnostic assessment before any injection is planned.
If you experience sudden weakness in both legs, loss of bladder or bowel control, or numbness in the groin area, seek emergency assessment immediately rather than booking an injection appointment. These symptoms may indicate cauda equina syndrome, a spinal emergency that requires urgent surgery.
What to Expect From an Injection Appointment
Most sciatica injections at Singapore Paincare are performed as outpatient procedures. You do not need a hospital stay. The procedure typically takes between fifteen and forty-five minutes, depending on the type and level of image guidance used.
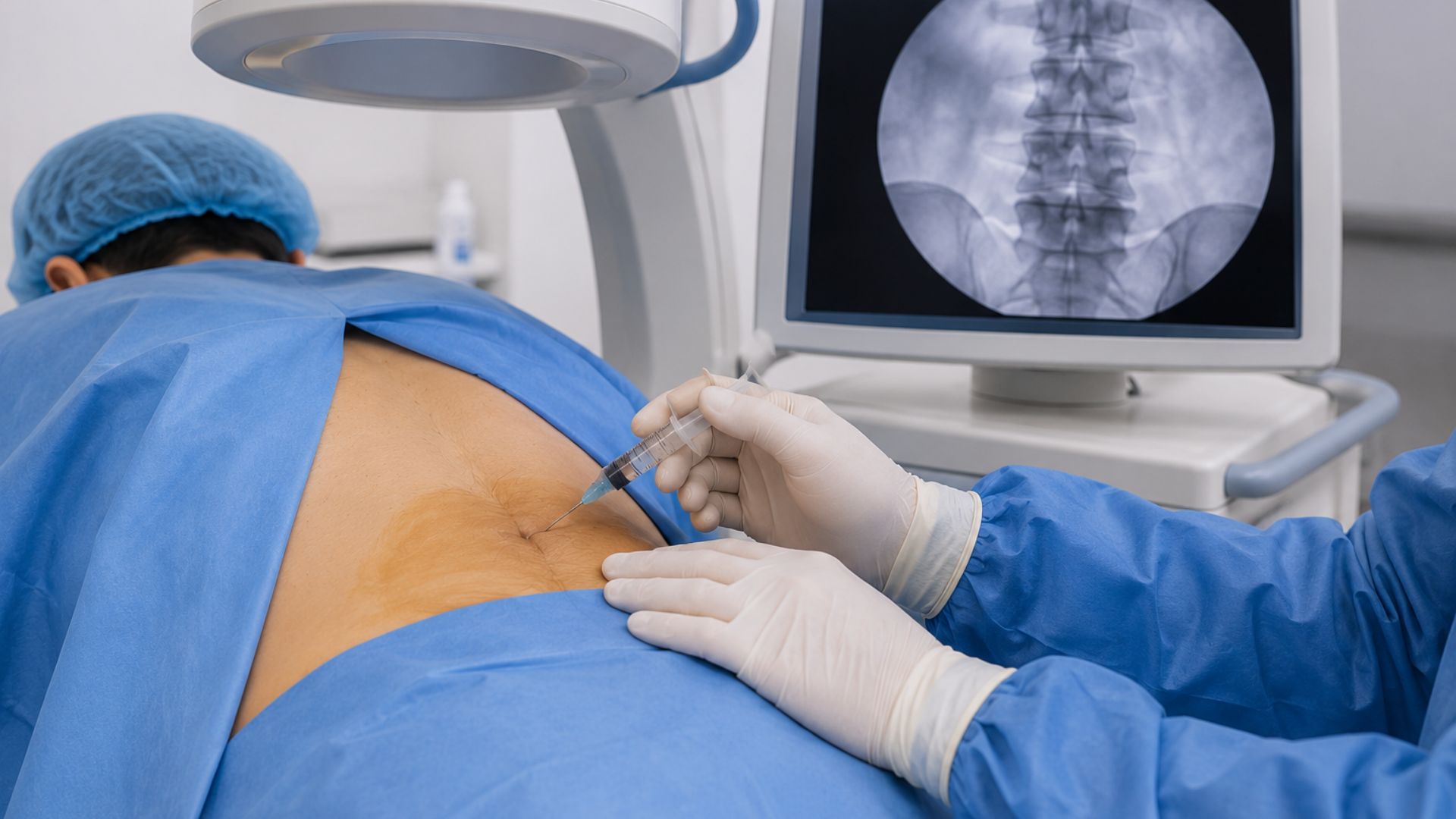
For epidural and nerve block procedures, a fine needle is guided under fluoroscopy (live X-ray) or ultrasound to the target site. A contrast dye may be used to confirm needle position before the medication is delivered. Local anaesthetic is given first to minimise discomfort. Most patients describe mild pressure or a brief sensation of nerve awareness during the procedure, rather than sharp pain.
After the injection, you will be observed for a short period before being discharged. Some patients notice immediate relief from the local anaesthetic component. The steroid component typically takes two to five days to produce its full anti-inflammatory effect. Light activity is usually possible the same day. Heavy lifting and strenuous exercise are avoided for a few days.
Some patients achieve lasting relief from a single procedure. Others benefit from a short course of two to three injections over several weeks. Your pain specialist will review your response and adjust the plan based on how you are progressing.
When Should You See a Specialist?
You do not need a referral to see a pain specialist in Singapore for your sciatica condition. If any of the following apply, a consultation to discuss an injection for sciatica is appropriate.
Your leg pain has lasted more than four to six weeks despite consistent conservative treatment. Your pain is severe enough to disrupt sleep, work, or daily activity. You have progressive leg weakness or numbness. You have been told surgery may be needed and want to understand your non-surgical alternatives. You have had injections before that provided only partial or temporary relief and want a more thorough diagnostic assessment before your next step.
Speak to a pain specialist to find out if an injection for sciatica is the right next step for your condition.
Conclusion
An injection for sciatica is a precisely targeted intervention that becomes appropriate when inflammation and nerve compression have reached a level that conservative care cannot manage adequately. The key to a good outcome is not simply choosing an injection, but choosing the right injection for the confirmed source of nerve irritation.
If sciatic pain is limiting your life in Singapore, book a consultation with the Singapore Paincare pain management team. A thorough assessment is the first step toward a treatment plan that addresses the actual source of your pain, not just its symptoms.
Read more: Sciatica
Frequently Asked Questions
How do I know if I need an injection for sciatica or just physiotherapy?
If your sciatica is improving with physiotherapy and the leg pain is manageable and getting better, physiotherapy alone may be sufficient. An injection for sciatica becomes appropriate when physiotherapy is not producing meaningful improvement after four to six weeks, when pain is too severe to do the exercises properly, or when nerve weakness or numbness is present. The two approaches are not mutually exclusive. An injection often makes physiotherapy possible again by reducing pain enough for movement.
How long does an injection for sciatica last?
The duration depends on the injection type and the individual patient. Epidural steroid injections typically provide relief for between six weeks and six months, with the strongest benefit in the first three months. Peripheral Nerve Blocks last from weeks to several months. Pulsed Radiofrequency tends to provide longer-lasting relief of three to twelve months. Nucleoplasty addresses the mechanical source of compression and can provide sustained relief in suitable patients. Your pain specialist will discuss realistic expectations based on your specific diagnosis.
Is an injection for sciatica painful?
Most patients tolerate the procedure well. Local anaesthetic is applied before the injection to minimise discomfort. Patients typically describe mild pressure or a brief awareness of the nerve during needle placement. Some temporary soreness at the injection site is normal for one to two days afterward. Significant post-procedure pain is uncommon.
Can sciatica injections be repeated?
Yes, most injection types can be repeated if the initial response was positive but relief has worn off. Epidural steroid injections are generally spaced at least four to six weeks apart. Pulsed Radiofrequency and nerve blocks can also be repeated. Your pain specialist will recommend a plan based on how you responded to the first treatment.
What is the difference between an epidural injection and a nerve block for sciatica?
An epidural injection delivers steroid medication into the epidural space, which is the area surrounding all the nerve roots as they exit the spinal cord at a given level. It treats inflammation across that region of the spine. A peripheral nerve block targets a single, specific nerve or nerve root with local anaesthetic and sometimes steroid. The nerve block is more precise, useful both for confirming which nerve is the source of pain and for treating a single nerve root or the sciatic nerve in the buttock. The choice depends on whether the goal is broader spinal anti-inflammation or precise single-nerve treatment.
Why did my previous sciatica injection stop working?
There are two common reasons. First, the injection may have been placed at the correct level but only addressed one driver of the pain. If sciatica has both a spinal component and a piriformis muscle component, an epidural alone will produce incomplete relief. Second, if the nerve has become sensitised over time, the pain is no longer driven primarily by inflammation. In this case, Pulsed Radiofrequency targets the nerve’s firing pattern directly, which is what is needed rather than another epidural. A fresh diagnostic assessment helps identify which situation applies.
About Singapore Paincare
Singapore Paincare Medical Group is a SGX-listed pain management group led by Consultant Pain Specialist Dr. Bernard Lee Mun Kam. With clinics at Paragon and Novena and a network of 18 locations island-wide, the group uses the Painostic® methodology to provide accurate diagnosis and minimally invasive treatment for a wide range of pain conditions. No referral is required.
Medical Disclaimer
This article is intended for general informational purposes only and does not constitute medical advice. Please consult a qualified healthcare professional for diagnosis and treatment tailored to your individual condition.