
Can Gout Cause Heel Pain?
June 22, 2026
CONTENTS
- What Is Gout? Understanding the Condition
- Can Gout Cause Heel Pain?
- Gout vs. Plantar Fasciitis — How to Tell the Difference
- Symptoms of Gout in the Heel
- When to See a Foot Pain Specialist
- How Gout in the Heel Is Diagnosed — The Painostic® Approach
- Treatment Options for Gout Heel Pain
- Self-Management Tips for Gout Heel Pain
- Speak to a Foot Pain Specialist in Singapore
- Frequently Asked Questions
Quick Answer:
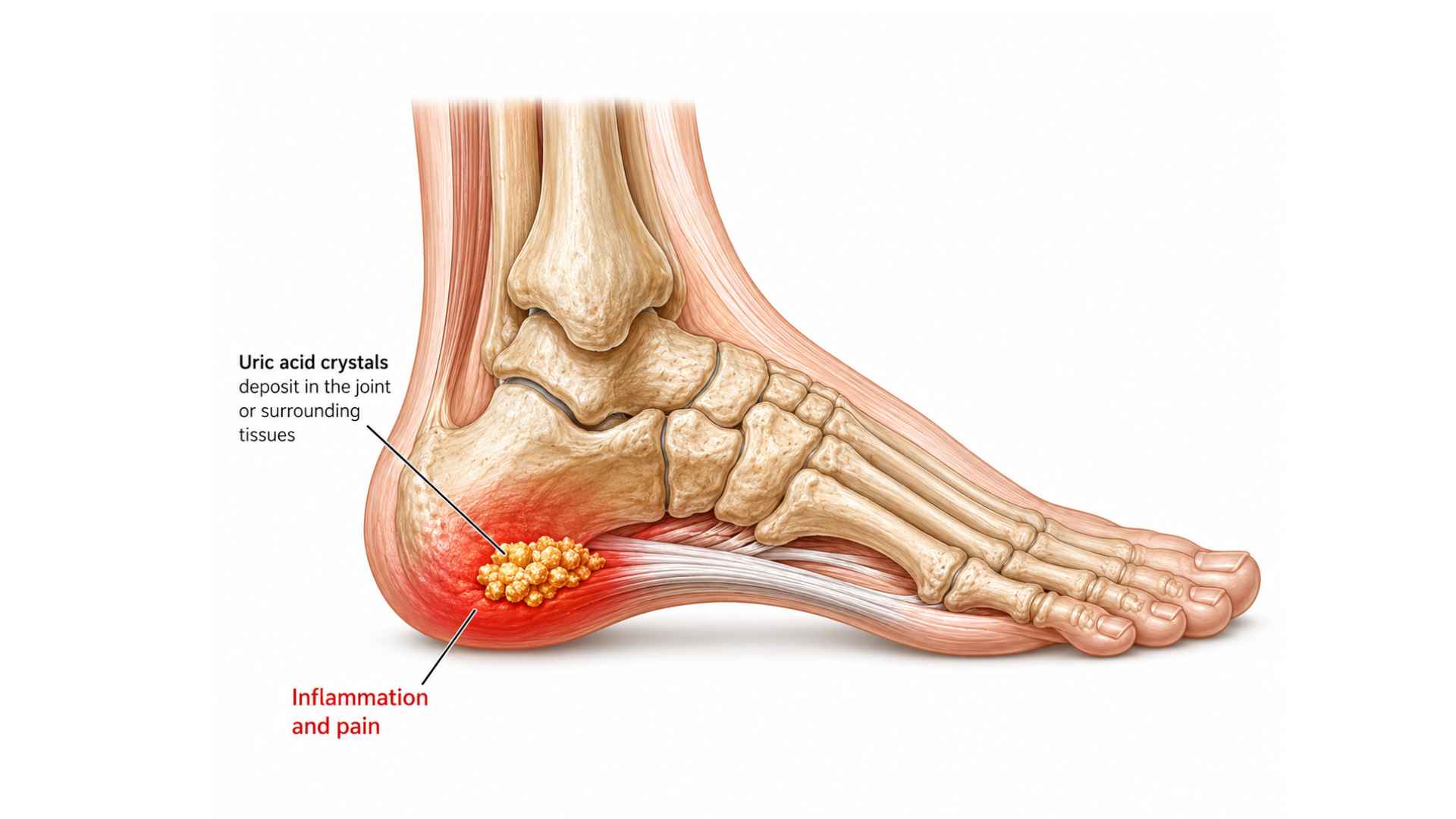
Yes — gout can cause heel pain. When uric acid crystals accumulate in the heel’s joints or surrounding soft tissue, they trigger an intense inflammatory response that produces sudden, severe pain, swelling, and warmth — often striking overnight with no warning. Gout-related heel pain is frequently mistaken for plantar fasciitis or Achilles tendinopathy, but it follows a distinct pattern and requires a different treatment approach.
If you have woken up to a throbbing, swollen heel with no clear explanation, you are not alone — and gout may be the reason. Most people associate gout with the big toe, but uric acid crystals can deposit in virtually any joint in the foot, including the structures around the heel. Without the right diagnosis, gout in the heel is often treated as a mechanical foot problem — meaning the true cause continues unchecked, and each attack gradually damages the joint further.
This article explains exactly how gout causes heel pain, how it differs from other common heel conditions, how it is properly diagnosed, and what treatment options are available in Singapore.
What Is Gout? Understanding the Condition
Gout is a form of inflammatory arthritis caused by the build-up of monosodium urate crystals in and around the joints. It develops when there is too much uric acid in the bloodstream — a condition called hyperuricaemia. Uric acid is a natural by-product of the body’s breakdown of purines, compounds found in many foods and produced naturally by cells. When the kidneys cannot clear uric acid fast enough, or when dietary load is too high, the excess crystallises in the cooler, peripheral joints of the body — most often the feet.
There are three recognised phases of gout:
- Acute gout flares — sudden, intense attacks of pain, swelling, redness, and warmth in a joint, typically lasting three to ten days
- Intercritical gout — the period between attacks where no symptoms are present but uric acid crystals remain in the joint, silently eroding tissue
- Chronic tophaceous gout — long-standing, poorly managed gout that leads to deposits of chalky white crystal nodules (tophi) in soft tissue and permanent joint damage
Singapore context: Gout is one of the most prevalent inflammatory arthritis conditions in Singapore. A cohort study published by the Singapore Family Physician reported a gout prevalence of 4.1% among Singaporean Chinese, based on a large cohort of over 52,000 adults — and Singapore ranks among the three highest age-standardised prevalence rates for gout in Asia (PLOS ONE, 2025). Risk is amplified by Singapore’s diet patterns, including regular consumption of seafood, organ meats, and alcohol — all high-purine foods that elevate uric acid levels. Men in their 40s are most commonly affected, though women’s risk rises significantly after menopause.
Can Gout Cause Heel Pain?
Yes — and it does so through several distinct mechanisms. The heel contains two structures that are particularly vulnerable to uric acid crystal deposits:
- The subtalar joint — where the heel bone (calcaneus) meets the ankle bone (talus)
- The area around the Achilles tendon insertion — where the tendon attaches to the back of the heel bone
When uric acid crystals accumulate in either location, the immune system recognises them as foreign bodies and launches a rapid inflammatory cascade. Understanding the specific mechanisms helps explain why gout heel pain feels different from other heel conditions.
Mechanism 1 — Crystal-Induced Joint Inflammation
Needle-shaped uric acid crystals lodge within the synovial lining of the subtalar joint. White blood cells rush in to engulf them, releasing inflammatory chemicals that cause intense swelling, heat, and pain within hours. Because the subtalar joint governs the side-to-side tilting motion of the foot, any inflammation here makes walking or placing weight on the heel almost impossible during a flare.
Mechanism 2 — Peritendinous Crystal Deposits
Uric acid crystals do not confine themselves to joints. They can accumulate in the soft tissue surrounding the Achilles tendon at its heel insertion. This triggers localised inflammation of the tendon sheath, producing a presentation that closely mimics Achilles tendinopathy — pain and stiffness at the back of the heel, particularly after rest. The key difference is that gout-related Achilles pain typically arrives suddenly and is disproportionately severe compared with tendon overuse injury.
Mechanism 3 — Bursa Involvement (Retrocalcaneal Bursitis)
Between the Achilles tendon and the heel bone sits a small fluid-filled sac called the retrocalcaneal bursa, designed to reduce friction. Uric acid crystals can infiltrate this bursa, causing it to become inflamed and swollen — a condition called gouty bursitis. This produces deep, posterior heel pain that worsens with direct pressure and with ankle flexion.
Mechanism 4 — Referred Pain and Altered Gait
Severe heel pain from any of the above mechanisms causes compensatory changes in how a person walks. Offloading the painful heel shifts weight unnaturally to other parts of the foot, placing excess stress on the arch, midfoot, and ankle. This can produce secondary pain in the plantar fascia, the midfoot joints, or the calf muscles — extending the pain beyond the heel itself and further complicating diagnosis.
Mechanism 5 — Peripheral Nerve Sensitisation
In chronic or recurrent gout, persistent crystal-induced inflammation can sensitise the nerves around the heel and ankle. This results in hypersensitivity where even light touch or a change in temperature causes pain — making the foot exquisitely tender even during the intercritical period between active flares.
Gout vs. Plantar Fasciitis — How to Tell the Difference
Gout heel pain is frequently confused with plantar fasciitis — the most common cause of heel pain. Both can cause significant morning heel pain, but they differ in important ways.
| Feature | Gout in the Heel | Plantar Fasciitis |
|---|---|---|
| Pain onset | Sudden, often overnight with no warning | Gradual, worsens over weeks |
| Pain character | Intense, burning, excruciating | Sharp, stabbing, or aching |
| Pain timing | Can be severe even at complete rest | Worst with first steps in the morning, improves with movement |
| Swelling & redness | Prominent — skin may be shiny and hot | Minimal or absent |
| Pain location | Back or side of heel, around Achilles | Bottom of heel, along arch |
| Duration | Days to weeks, then resolves | Persistent without treatment |
| Triggers | Rich food, alcohol, dehydration, illness | Overuse, poor footwear, prolonged standing |
| Affected individuals | More common in middle-aged men | Runners, people on their feet all day, those with flat arches |
| Blood findings | Elevated serum uric acid | Normal uric acid levels |
| Response to NSAIDs | Dramatic improvement | Moderate improvement |
Important: These two conditions can coexist. Some patients have both plantar fasciitis and gouty inflammation in the same foot, which complicates diagnosis. A clinical assessment — including blood tests and imaging — is essential to determine the correct cause before treatment is started.
Symptoms of Gout in the Heel
Gout-related heel pain follows a recognisable pattern. You may notice:
- Sudden, severe pain in the heel or back of the foot, often arriving overnight or in the early morning without any preceding injury
- Pronounced swelling around the heel joint, ankle, or Achilles tendon insertion
- Redness and warmth — the skin over the affected area may appear shiny and feel noticeably hot to the touch
- Extreme tenderness — even the light pressure of a bedsheet can feel intolerable
- Limited range of motion — difficulty flexing or extending the ankle, or bearing weight on the foot
- Resolution between attacks — after several days, pain subsides completely, only to return weeks or months later, often with greater intensity
- Tophi formation (in chronic cases) — firm, white nodules developing under the skin around the heel or Achilles tendon, indicating long-standing crystal deposits
When nerve involvement is suspected: If you experience burning, tingling, or numbness extending into the sole of the foot or the toes during a flare, this may indicate that the inflammatory process is affecting nearby nerves — and warrants prompt specialist assessment.
When to See a Foot Pain Specialist
Do not dismiss recurring heel pain as a minor inconvenience. Seek specialist assessment if:
- Heel pain arrives suddenly and severely, with no clear mechanical cause such as a recent injury or overuse
- You notice visible swelling, redness, or warmth around the heel or ankle during a pain episode
- You have a known diagnosis of gout elsewhere in the body and now experience heel pain
- Heel pain episodes resolve on their own but keep returning — with each attack potentially more severe than the last
- You have metabolic risk factors such as obesity, hypertension, diabetes, or chronic kidney disease, which increase gout risk
- Over-the-counter anti-inflammatory medication provides significant relief but the pain returns after it wears off
Early diagnosis prevents joint damage. Repeated gout flares that go untreated — even if pain resolves between episodes — continue to deposit crystals that erode cartilage and bone. By the time tophi are visible, significant irreversible damage may already have occurred.
How Gout in the Heel Is Diagnosed — The Painostic® Approach
Diagnosing gout heel pain requires more than a uric acid blood test. At Singapore Paincare, our pain specialists use the Painostic® methodology — a structured, three-protocol assessment designed to identify the true source of your pain before any treatment begins.
Diagnostic Formulation
A multi-dimensional assessment covering your full pain history, physical examination, imaging findings, and validated pain questionnaire. For suspected gout, this includes evaluation of flare pattern, dietary and lifestyle triggers, metabolic comorbidities, and family history. The assessment differentiates mechanical heel pain from crystal-induced inflammatory pain, and evaluates all potential pain generators — including the subtalar joint, Achilles tendon insertion, retrocalcaneal bursa, and surrounding nerve structures. Where imaging is indicated, ultrasound can detect crystal deposits and joint effusion; joint aspiration and synovial fluid analysis remains the definitive test, identifying uric acid crystals under polarised light microscopy. Goal: pinpoint the exact source before any treatment decision is made.
Injection Roadmap
Once the pain source is identified, a structured, evidence-based treatment plan is developed — combining minimally invasive procedures, physical therapy, and pharmacotherapy in a sequence tailored to the specific condition. For gout heel pain, this roadmap addresses both the acute inflammatory episode and the longer-term goal of uric acid reduction, with procedures targeted to the confirmed pain generators.
Injection Technique
Refined techniques determine precise needle depth and optimal placement to ensure medication is delivered accurately to the affected anatomical structure — whether that is the subtalar joint, the retrocalcaneal bursa, or the peritendinous soft tissue. Image guidance ensures precision and reduces the risk of inadvertent soft tissue damage.
Where the pain source remains unclear, image-guided diagnostic nerve blocks can be used to confirm the precise pain generator. Treating the wrong structure — for example, applying plantar fasciitis physiotherapy to a joint that is actually inflamed by gout crystals — will not resolve the underlying condition and risks allowing continued joint damage while the patient believes they are being treated appropriately.
Treatment Options for Gout Heel Pain
Conservative Management
The following approaches form the foundation of gout heel pain management and are appropriate for mild-to-moderate presentations or as adjuncts to minimally invasive care:
- Urate-lowering therapy (ULT): Medications such as allopurinol or febuxostat reduce the production or enhance the excretion of uric acid, lowering blood levels over time to prevent future crystal formation. ULT is a long-term commitment — stopping medication prematurely is a common cause of recurrent flares.
- Anti-inflammatory pharmacotherapy: During acute flares, NSAIDs, colchicine, or corticosteroids may be prescribed to bring inflammation under control rapidly.
- Dietary and lifestyle modification: Reducing purine-rich foods (red meat, organ meats, shellfish, beer), increasing hydration, limiting alcohol, and maintaining a healthy weight all help reduce uric acid levels.
- Rest and off-loading: During acute flares, reducing weight-bearing on the affected heel accelerates recovery and prevents worsening of joint inflammation.
Minimally Invasive Procedures
When conservative measures are insufficient to control pain, or when structural joint damage requires direct intervention, Singapore Paincare’s specialists offer a range of minimally invasive procedures tailored to the heel pain source.
MYOSPAN — Joint and Soft Tissue Procedures
| Procedure | How It Helps |
|---|---|
| Intra-Articular Injections | Anti-inflammatory agents delivered directly into the subtalar joint to reduce crystal-induced inflammation, relieve pain, and restore joint mobility. |
| Coreflex Injections | A combination of local anaesthetic, anti-inflammatory, and muscle relaxant delivered to the affected peritendinous or bursal tissue to break the inflammatory pain cycle. |
| Platelet-Rich Plasma (PRP) | Uses the patient’s own platelets to support tissue repair in areas where repeated gout flares have caused localised soft tissue damage around the heel. |
NEUROSPAN — Nerve-Targeted Procedures
| Procedure | How It Helps |
|---|---|
| Peripheral Nerve Block | Local anaesthetic and anti-inflammatory agents injected around specific nerves at the heel to interrupt pain signals and confirm the nerve as a pain generator. |
| Pulsed Radiofrequency (PRF) | Low-temperature radiofrequency energy desensitises overactive pain-signalling nerves around the heel without ablation, providing longer-term relief from chronic gout-related nerve hypersensitivity. |
Singapore Paincare has provided minimally invasive pain treatments as alternatives to open surgery for over a decade. All procedures are performed on an outpatient or day-surgery basis — no hospital admission required.
Self-Management Tips for Gout Heel Pain
- Stay well hydrated — Aim for at least two litres of water daily. Adequate hydration helps the kidneys flush uric acid more efficiently, reducing the concentration in your bloodstream and the risk of crystal formation.
- Review your diet — Limit high-purine foods such as red meat, organ meats (liver, kidney), shellfish, and beer. You do not have to eliminate them entirely, but reducing portion sizes and frequency can make a meaningful difference to your uric acid levels over time.
- Do not stop your urate-lowering medication — A common mistake is discontinuing allopurinol or similar medication when symptoms improve. Stopping ULT too early causes uric acid to rise again, triggering a new flare. Take medication as prescribed and discuss any concerns with your doctor.
- Protect your heel during a flare — Rest the foot, elevate it above heart level when sitting or lying down, and apply an ice pack wrapped in a cloth for 15–20 minutes at a time to reduce swelling. Avoid walking barefoot on hard floors.
- Monitor for gout in other joints — Gout rarely stays confined to one location over a lifetime. If you notice sudden pain in the knee, ankle, wrist, or elbow — particularly after a known dietary trigger — consider whether gout may also be affecting those joints and seek assessment early.
Speak to a Foot Pain Specialist in Singapore
Persistent or recurring heel pain that strikes suddenly, especially with swelling and redness, deserves a proper clinical assessment — not a wait-and-see approach. At Singapore Paincare, our pain specialists assess all potential causes of heel pain, including gout, using the Painostic® methodology to build a multi-dimensional picture of your condition before recommending any treatment. Whether your heel pain turns out to be gout, plantar fasciitis, Achilles tendinopathy, or a combination of conditions, our team will identify the source accurately and map out a personalised, minimally invasive treatment plan tailored to you.
Frequently Asked Questions
Can gout really cause heel pain, or is it always in the big toe?
While the big toe is the most common site for gout — affecting roughly 75% of patients at some point — gout can occur in any joint where uric acid crystals accumulate. The heel, specifically the subtalar joint and the tissue around the Achilles tendon insertion, is a well-documented site for gout deposits. Research has found that around 35% of gout patients experience pain in the posterior heel at some stage of their condition.
How do I know if my heel pain is gout or plantar fasciitis?
The clearest distinguishing features are the onset and behaviour of the pain. Plantar fasciitis develops gradually and is worst with your very first steps in the morning, then eases with movement. Gout heel pain typically arrives suddenly — often overnight with no prior warning — is severe even at complete rest, and is accompanied by visible redness and swelling. Blood tests for serum uric acid and ultrasound imaging can help confirm the diagnosis. Because the two conditions can coexist, a specialist assessment is always recommended.
Does recurring heel pain mean my gout is getting worse?
More frequent or more severe flares are a sign that uric acid levels are not being adequately controlled. Even in the pain-free periods between attacks, crystals remain in the joint and continue causing microscopic damage. Without proper uric acid management, attacks tend to become more frequent, last longer, and eventually lead to chronic joint changes — including tophi formation and permanent cartilage loss.
Can minimally invasive procedures help gout-related heel pain?
Yes. When conservative management is insufficient — or when an acute flare is severely debilitating — targeted injections into the subtalar joint or surrounding soft tissue can provide rapid pain relief. Procedures such as intra-articular anti-inflammatory injections, Coreflex injections, and image-guided nerve blocks address the specific inflammatory source rather than the symptom alone. These are performed on an outpatient basis with minimal downtime.
Will I need surgery for gout in my heel?
Surgery is rarely required for gout heel pain. The vast majority of cases respond to a combination of uric acid-lowering medication, dietary modification, and targeted minimally invasive procedures when needed. Surgery may be considered in very advanced cases where large tophi have destroyed joint structure or are compressing nearby nerves — but this represents a late-stage outcome that is largely preventable with early diagnosis and consistent treatment.
Where can I see a foot pain specialist for gout in Singapore?
Singapore Paincare Medical Group’s pain specialists see patients presenting with gout-related heel pain and other complex foot pain conditions at:
Singapore Paincare Center @ Paragon — 290 Orchard Road #18-03, Singapore 238859
Singapore Paincare Center @ Novena — 38 Irrawaddy Road #07-33, Singapore 329563
No referral is required. Appointments can be booked directly at either clinic.
Key Takeaways
- Gout is a form of inflammatory arthritis caused by uric acid crystal deposits — and it can affect the heel, not just the big toe, causing sudden and severe pain that is often mistaken for plantar fasciitis.
- Heel gout primarily targets the subtalar joint and the Achilles tendon insertion, triggering an acute inflammatory response that produces intense swelling, warmth, and tenderness within hours.
- Distinguishing gout from plantar fasciitis is essential: gout arrives suddenly, is severe at rest, and comes with visible redness and swelling — features not typically associated with mechanical heel pain.
- Untreated gout causes progressive, cumulative joint damage even during symptom-free intervals — making early diagnosis and uric acid management critical, not optional.
- The Painostic® diagnostic methodology at Singapore Paincare uses a structured three-protocol assessment to accurately identify the source of heel pain before any treatment is selected — ensuring that the right structure is treated, not the wrong one.
References
- Singapore Family Physician — 4.1% gout prevalence among Singaporean Chinese, based on a cohort of 52,332 adults aged 45–74 years (2012 study cited in CFPS publication)
- Frontiers in Medicine — Gout prevalence of 4.1% among Singaporean Chinese; only 22.3% of local patients achieved serum uric acid targets in a Singapore primary care cohort study (PMC10513174, 2023)
- PLOS ONE — Singapore ranked among the three highest age-standardised prevalence rates for gout in Asia in 2021, at 805.67 per 100,000 population (2025 publication)
- Achilles Foot and Ankle Center — Clinical description of uric acid crystal accumulation in the subtalar joint and Achilles tendon insertion as mechanisms of heel gout (achillesfootandankle.com, 2026)
- Liv Hospital / International Clinical Review — Approximately 35.1% of gout patients experience posterior heel pain; mechanistic explanation of uric acid crystallisation in peripheral, cooler joints (int.livhospital.com, 2026)
- American College of Rheumatology — 2020 Gout Management Guidelines; allopurinol recommended as first-line urate-lowering therapy for all eligible patients
- DigitalHealth.sg — Gout noted as the most common inflammatory arthritis in Singapore; Healthier SG Primary Care estimated local prevalence of 4.1% (2026)
This article is intended for general informational purposes only and does not constitute medical advice. Please consult a qualified healthcare professional for diagnosis and treatment tailored to your individual condition.