
Bone Spur vs Plantar Fasciitis: What Is Really Causing Your Heel Pain?
June 18, 2026
CONTENTS
- Understanding the Plantar Fascia and Why Heel Pain Is So Common
- What Is a Bone Spur (Heel Spur)?
- Bone Spur vs Plantar Fasciitis: The Key Differences
- Interpreting Your Heel Pain by Location and Timing
- Red Flag Symptoms That Require Prompt Attention
- How Is Bone Spur vs Plantar Fasciitis Diagnosed?
- Bone Spur vs Plantar Fasciitis Treatment in Singapore: What Are Your Options?
- Treating Plantar Fasciitis
- Treating a Symptomatic Bone Spur
- A Pain Specialist’s Perspective
- Managing Heel Pain Day-to-Day: Practical Advice
- When Should You See a Foot Pain Specialist in Singapore?
- Conclusion
Quick Answer:
Bone spurs and plantar fasciitis are two conditions that are frequently confused because they often occur together. Plantar fasciitis is inflammation of the thick band of tissue connecting your heel to your toes. A bone spur is a calcium deposit that forms on the heel bone in response to chronic stress. While both can cause heel pain, it is the inflamed tissue, not the spur itself, that is usually responsible. Accurate diagnosis by a foot pain specialist is the first step toward the right treatment.
You wake up in the morning, swing your legs out of bed, take your first step, and feel a sharp stab of pain shoot through your heel. You reach for your phone, type in your symptoms, and are met with two possible culprits: plantar fasciitis and bone spurs. The two names appear side by side so often that many patients assume they are the same condition or that one always causes the other.
They are not the same, and the distinction matters enormously for treatment.
Bone spur vs plantar fasciitis is one of the most common diagnostic questions our foot pain specialists see in Singapore. Patients come in having been told by a friend, a general practitioner, or even a radiology report that they have a heel spur, only to discover that the spur itself is not actually causing their pain. Others believe their plantar fasciitis will resolve on its own, not realising they have been dealing with a structural problem that needs targeted treatment.
This article walks you through the key differences between the two conditions, what each one actually involves, and how a proper clinical assessment helps identify the right path forward.
Understanding the Plantar Fascia and Why Heel Pain Is So Common
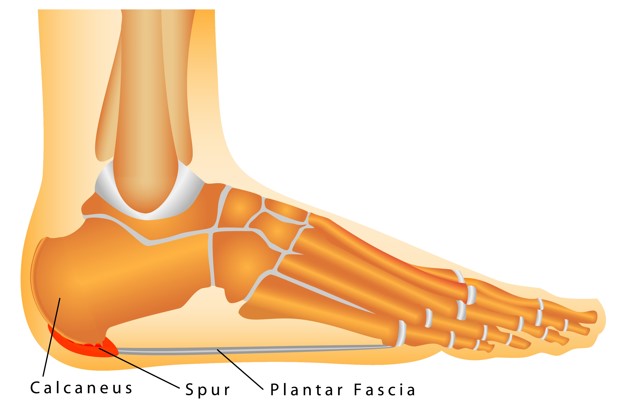
The plantar fascia is a thick band of fibrous tissue that runs along the sole of your foot, connecting your heel bone (calcaneus) to the base of your toes. It acts as a natural shock absorber, supporting the arch of your foot with every step you take. When you walk, run, or stand for long periods, this band stretches and contracts repeatedly, bearing a significant share of your body weight.
According to the SingHealth Duke-NUS Sport and Exercise Medicine Centre, approximately 10% of the general population is expected to develop plantar fasciitis at some point in their lifetime (Annals of the Academy of Medicine, Singapore, 2024). In Singapore, this risk is heightened by several local factors: flat feet are more common among Asian populations, the widespread use of unsupportive slippers and sandals places extra strain on the fascia, and many Singaporeans spend long hours on hard, tiled surfaces at home, in hawker centres, or on the job.
When the plantar fascia is repeatedly stressed beyond its capacity, microscopic tears develop at the point where the tissue meets the heel bone. The body responds with inflammation, which is the hallmark of plantar fasciitis.
What Is a Bone Spur (Heel Spur)?
A bone spur, also called a heel spur or calcaneal spur, is a small deposit of calcium that builds up on the underside of the heel bone. It develops gradually over months or years as the body attempts to reinforce an area of chronic stress. Think of it as the skeleton’s version of building a callus: repeated tension at the point where the plantar fascia meets the heel stimulates new bone growth.
The key fact that surprises most patients is this: bone spurs very rarely cause pain on their own. Research consistently shows that only about 5% of people with heel spurs experience pain attributable to the spur itself (American Academy of Orthopaedic Surgeons). The vast majority of heel spurs are silent. They appear incidentally on X-rays taken for another reason, and the patient has no symptoms at all.
Published research shows that a plantar calcaneal spur is present in approximately 73% of patients who present with heel pain (Shama et al., cited in Menz et al., Journal of Foot and Ankle Research, 2008), yet spurs are also found in a significant proportion of people with no symptoms at all. This means the presence of a spur on an X-ray cannot, on its own, explain a patient’s pain. The confusion arises when both a heel spur and heel pain appear on the same imaging report, leading the patient, and sometimes the treating doctor, to assume the spur is the problem. In most cases, it is the inflamed fascia that is driving the pain, not the bony growth.
Bone Spur vs Plantar Fasciitis: The Key Differences
Understanding bone spur vs plantar fasciitis comes down to understanding what is inflamed versus what has calcified.
Plantar fasciitis is a soft tissue condition. The pain comes from an inflamed, micro-torn band of tissue. It is typically felt along the inner heel and into the arch, worsens after rest, and is aggravated by pressing firmly on the base of the heel. Ultrasound or MRI will show thickening and signal changes in the fascia itself.
A bone spur is a structural change in the bone. It is visible on X-ray as a small hook-like projection on the front or underside of the calcaneus. Because most spurs produce no symptoms, the diagnosis of “painful heel spur” is only made when a clinician can rule out all other sources of heel pain and confirm that the spur is mechanically causing symptoms, which is comparatively uncommon.
Both conditions can coexist, and in patients with long-standing plantar fasciitis, a bone spur may develop as a secondary consequence of chronic inflammation at the heel attachment. Studies suggest that up to half of people with chronic plantar fasciitis also have heel spurs, though in these cases it is still typically the fascia inflammation driving the pain.
One practical distinction worth noting: if your heel pain appeared overnight, if it is associated with swelling, redness, or warmth, or if the pain is affecting both heels simultaneously, these features point toward different diagnoses entirely, such as gout, Achilles tendinopathy, or a systemic inflammatory arthritis. A specialist assessment can rule these out quickly.
Interpreting Your Heel Pain by Location and Timing
Where exactly your pain sits on the heel can offer useful clues about its origin, though it cannot replace a proper clinical assessment.
Pain centred directly on the inner base of the heel, worst with the first morning steps and improving with gentle walking, fits the classic plantar fasciitis presentation. If you can find a precise tender spot by pressing your thumb firmly into the inner edge of your heel, close to where the arch begins, this is often the site of fascia attachment and suggests plantar fasciitis as the primary diagnosis.
Pain at the back of the heel, close to where the Achilles tendon meets the bone, points more toward Achilles tendinopathy or a posterior heel spur, which is a different condition from the plantar-surface spur associated with plantar fasciitis.
Pain that radiates upward into the calf, or that is accompanied by tingling or numbness in the foot, may suggest nerve involvement rather than pure fascia pathology. Tarsal tunnel syndrome, which is a compression of the tibial nerve at the ankle, is sometimes mistaken for plantar fasciitis because it also produces inner heel pain.
Heel pain that is diffuse, hard to localise precisely, or associated with stiffness in multiple joints should prompt investigation for inflammatory conditions. The key message is this: location matters, but so does the full clinical picture. Do not rely on self-diagnosis to determine which condition you have
Red Flag Symptoms That Require Prompt Attention
Most heel pain has a mechanical or degenerative cause and is not dangerous. However, some presentations warrant urgent assessment:
- Sudden, severe heel pain following a jump or a fall, which may indicate a stress fracture or plantar fascia rupture
- Heel pain accompanied by fever, redness, or warmth, which can signal infection
- Bilateral heel pain with associated lower back stiffness in a younger person, which may indicate ankylosing spondylitis
- Persistent heel pain that does not improve at all after six to eight weeks of rest and conservative care
- Unexplained weight loss combined with bone pain, which requires investigation to exclude bone pathology
If any of these features apply to you, seek a clinical assessment promptly rather than waiting to see if the pain resolves on its own.
How Is Bone Spur vs Plantar Fasciitis Diagnosed?
Accurate diagnosis is the foundation of effective treatment. At Singapore Paincare, our specialists use the Painostic methodology, a proprietary four-pillar diagnostic framework developed by Dr Bernard Lee, to assess heel pain from multiple dimensions rather than relying on imaging alone.
The assessment begins with a detailed pain history. How long have you had the pain? What makes it worse and what gives relief? Does it hurt more after activity or during it? Is the pain sharp and localised, or diffuse and aching? These patterns help differentiate plantar fasciitis from bone spur pain, nerve entrapment, and other causes.
Physical examination then involves careful palpation of the heel and arch to identify the precise tender point. The Windlass test, which involves dorsiflexing (bending upward) the big toe while the foot bears weight, can reproduce plantar fasciitis pain and help confirm the diagnosis. The degree of ankle flexibility and calf muscle tightness are also assessed, as tight calf muscles are one of the most common contributors to persistent plantar fasciitis.
Imaging completes the picture. An X-ray is useful for visualising bone spurs, ruling out fractures, and assessing the overall structure of the heel. Ultrasound is particularly valuable for evaluating the plantar fascia directly, measuring its thickness, and confirming areas of inflammation or micro-tearing. MRI may be recommended when the diagnosis is unclear or when a partial fascia tear is suspected. Diagnostic injections can also serve a dual diagnostic and therapeutic role.
This multi-dimensional approach ensures that treatment is directed at the actual source of pain rather than at incidental findings on an X-ray.
Bone Spur vs Plantar Fasciitis Treatment in Singapore: What Are Your Options?
The most important principle in treating heel pain is this: the treatment must match the diagnosis. Because bone spurs and plantar fasciitis are structurally different problems, they respond to different interventions. A spur visible on X-ray does not automatically warrant treatment. The inflamed fascia, if present, almost always does.
At Singapore Paincare, our foot pain specialist team in Singapore takes a diagnosis-first approach using the Painostic methodology. The treatment roadmap is only drawn after the true source of pain has been identified through a multi-dimensional clinical assessment.
Treating Plantar Fasciitis
Plantar fasciitis is a soft tissue condition driven by inflammation and micro-tearing of the fascia. Treatment is therefore aimed at reducing inflammation, offloading the fascia, restoring tissue health, and correcting the mechanical factors that caused the problem in the first place. Most patients improve with a combination of conservative and, where needed, minimally invasive interventional care.
Activity Modification and Rest
Reducing activities that repetitively load the heel is an important first step. This does not mean complete rest, which can weaken the supporting structures of the foot. Low-impact activity such as swimming or cycling helps maintain fitness while the fascia is given the opportunity to recover.
Footwear Optimisation and Orthotics
Supportive footwear with adequate arch support and cushioned heels reduces the mechanical strain placed on the plantar fascia with every step. Patients are advised to avoid flat-soled shoes, worn-out trainers, and unsupported flip-flops, all common in Singapore’s casual lifestyle. Custom or off-the-shelf orthotic insoles can redistribute load more evenly across the sole, particularly for patients with flat feet or high arches.
Physiotherapy and Stretching
Targeted stretching of the calf muscles and plantar fascia is one of the most clinically effective conservative treatments for plantar fasciitis. Tight calf muscles increase the tension on the fascia at the heel attachment, so addressing this directly often produces significant relief. A physiotherapy programme also strengthens the intrinsic foot muscles and guides a gradual return to full activity.
Anti-Inflammatory Medication
Non-steroidal anti-inflammatory drugs (NSAIDs) such as diclofenac or celecoxib can help manage the acute inflammatory phase. These are typically used as a short-term measure while other treatments take effect rather than as a long-term solution.
Coreflex Injections
For patients whose plantar fasciitis persists despite conservative care, Coreflex Injections offer a more targeted option. This Myospan procedure delivers a precise combination of local anaesthetic, anti-inflammatory agent, and muscle relaxant directly to the affected fascia at the heel attachment, breaking the cycle of spasm and inflammation that perpetuates chronic pain. It is particularly appropriate for patients who have had symptoms for several months and have not responded to stretching and footwear changes alone.
Platelet-Rich Plasma (PRP) Therapy
Platelet-Rich Plasma (PRP) Therapy is the preferred regenerative option for chronic or degenerative plantar fasciitis, where the fascia has developed structural changes beyond simple acute inflammation. A small amount of the patient’s own blood is processed to concentrate healing growth factors, then injected precisely into the damaged tissue to stimulate repair and regeneration. PRP Therapy is particularly relevant for patients with long-standing symptoms or those who have not responded to corticosteroid injections and wish to avoid the tissue-weakening risks associated with repeated steroid use.
Peripheral Nerve Block
When plantar fasciitis is accompanied by a significant nerve component, including tingling, burning, or hypersensitivity around the inner heel, a Peripheral Nerve Block may be needed alongside fascia-directed treatment. This Neurospan procedure delivers local anaesthetic and anti-inflammatory medication around the specific nerve branches supplying the heel, interrupting pain signalling and reducing peripheral sensitisation. It can also serve a diagnostic role, confirming how much of the patient’s pain is nerve-driven versus fascia-driven.
Treating a Symptomatic Bone Spur
The key clinical point is that most bone spurs do not require any treatment at all. A spur that is incidentally discovered on X-ray, with no localised point tenderness directly over the bony prominence and no pain pattern that correlates to its position, is typically left alone. Treating it will not resolve heel pain if the fascia is the underlying driver.
A bone spur is only considered symptomatic when a specialist has ruled out plantar fasciitis and other causes, and can identify that the spur itself is mechanically contributing to pain, for example by directly impinging on surrounding soft tissue or nerves. In these cases, the treatment approach differs from plantar fasciitis management in several important ways.
Load Reduction and Padding
Offloading the specific area of bony contact is the first conservative step. Heel cups and silicone padding help redistribute pressure away from the spur during walking and standing. Unlike plantar fasciitis stretching programmes, aggressive calf and fascia stretching is less central to spur management, since the structural problem is osseous rather than inflammatory soft tissue.
Intra-Articular Injections and Targeted Anti-Inflammatory Treatment
When a spur is causing local tissue irritation, a targeted anti-inflammatory injection can reduce the reactive inflammation around the bony prominence. Intra-articular Injections deliver anti-inflammatory agents and, where appropriate, hyaluronic acid to the affected area to reduce pain, lower inflammation, and restore comfort during movement. This is not the same as a standard plantar fasciitis injection: the target site, depth, and clinical rationale differ based on the spur’s location and its relationship to surrounding structures.
Radiofrequency Ablation (RFA)
For patients with a truly symptomatic spur that has not responded to conservative measures, Radiofrequency Ablation may be considered. This Neurospan procedure uses controlled radiofrequency energy to disrupt the pain signals transmitted by the nerves in the immediate vicinity of the spur, reducing the chronic pain that the bony prominence is generating. RFA can provide long-lasting relief without the need for surgical removal of the spur, which is rarely indicated and carries its own recovery burden.
When Is Spur Removal Considered?
Surgical removal of a heel spur is uncommon and is considered only when a spur is definitively confirmed as the structural source of pain, all conservative and minimally invasive options have been exhausted, and the mechanical impingement is severe enough to warrant operative intervention. It is not a first-line treatment and should never be pursued based on an X-ray finding alone. Most patients with genuine spur-related symptoms achieve adequate relief through the non-surgical options above.
A Pain Specialist’s Perspective
One of the most common clinical mistakes I see in heel pain management is treating the X-ray rather than the patient. A heel spur on an image generates immediate concern. Patients come in having been told they have a spur, worried they may need surgery to remove it, when in reality the spur has nothing to do with their pain. Meanwhile, the actual driver of their symptoms, an inflamed and partially torn plantar fascia, has gone unaddressed for months.
There is also a more subtle clinical pattern that we see frequently among middle-aged Singaporean patients, particularly those in desk-bound jobs. They spend long hours sitting, then compensate with brisk walking or runs along the park connector at weekends, often in footwear that offers minimal support. The plantar fascia is not conditioned for the sudden mechanical load. Over weeks, inflammation builds at the heel attachment, but because the pain eases during the work day when they are seated, patients often underestimate its severity and delay seeking help.
By the time they see a specialist, many of these patients have had symptoms for six months or longer. At this stage, the fascia has often developed structural changes including thickening and early degenerative changes rather than simple acute inflammation. This distinction matters clinically because chronic degenerative plantar fasciitis responds differently from acute plantar fasciitis. Regenerative approaches such as PRP Therapy tend to be more appropriate at this stage than simple anti-inflammatory injections.
The message is this: if your heel pain has not responded to rest and stretching within four to six weeks, a specialist assessment is warranted. Early intervention prevents the cascade from acute inflammation to chronic structural change.
Managing Heel Pain Day-to-Day: Practical Advice
Patients with plantar fasciitis often find that consistent daily habits make a meaningful difference to their symptoms between treatment sessions. Stretching the calf and plantar fascia before getting out of bed in the morning, rather than placing sudden weight on a cold, contracted fascia, is one of the most effective self-management strategies. Night splints, which hold the foot in gentle dorsiflexion overnight, can also reduce morning pain by preventing the fascia from fully contracting during sleep.
Wearing supportive shoes from the moment your feet touch the floor matters more than most patients realise. Walking to the bathroom in flat slippers or on bare tiles immediately after waking up is the single most common trigger for severe morning heel pain in Singapore. Keeping a pair of supportive shoes or sandals beside the bed is a simple change that many patients say produces noticeable improvement within days.
Ice applied to the heel for 15 to 20 minutes after activity can help manage post-activity inflammation. Gentle self-massage using a frozen water bottle or a small ball rolled under the arch can also provide temporary relief.
These are supportive measures, not substitutes for a proper diagnosis. If your symptoms persist or worsen despite these strategies, seek a clinical assessment.
When Should You See a Foot Pain Specialist in Singapore?
Most cases of plantar fasciitis will improve with conservative care within a few months, but there are clear signs that a specialist opinion is needed sooner.
You should consider consulting a foot pain specialist if your heel pain has persisted for more than four to six weeks without improvement, if the pain is severe enough to change the way you walk, if you have already tried rest and stretching without meaningful relief, or if the pain is affecting your sleep, your work, or your ability to exercise. You do not need a referral from a general practitioner to see a pain specialist in Singapore.
A specialist can confirm whether your pain is due to plantar fasciitis, a bone spur, nerve entrapment, or another cause entirely, and offer a structured treatment plan tailored to your presentation.
Book a consultation with our foot pain specialist team at Singapore Paincare to take the first step toward a clearer diagnosis and a personalised treatment plan.
Conclusion
Heel pain is one of the most common musculoskeletal complaints in Singapore, and the confusion between bone spur vs plantar fasciitis is understandable. Both conditions involve the heel and can appear together on imaging reports. But they are distinct, and treating the wrong one wastes time and prolongs suffering.
Plantar fasciitis is an inflamed, micro-torn fascia that needs targeted conservative and, where appropriate, interventional treatment. A bone spur is usually a silent bystander on an X-ray, rarely the direct cause of pain. Getting this distinction right starts with a proper clinical assessment, not with an X-ray report alone.
If your heel pain has not responded to simple measures, speak to a pain specialist to find out what is actually driving your symptoms. Book a consultation with our pain management team at Singapore Paincare today.
Read More: Plantar Fasciitis
Frequently Asked Questions
What is the main difference between a bone spur and plantar fasciitis?
Plantar fasciitis is inflammation of the plantar fascia, the thick band of tissue connecting the heel bone to the toes. A bone spur is a calcium deposit that forms on the heel bone, usually in response to chronic stress at the same site. While they frequently co-exist, most bone spurs do not cause pain on their own. It is typically the inflamed fascia that is responsible for heel pain, even when a spur is visible on X-ray. Accurate diagnosis requires clinical assessment, not just imaging.
Can plantar fasciitis go away on its own?
Mild cases of plantar fasciitis can improve with rest, stretching, and footwear changes, particularly when caught early. However, the condition does not reliably resolve on its own, especially if the contributing factors, such as tight calf muscles, flat feet, or unsuitable footwear, are not addressed. Many patients find that symptoms fluctuate, easing for a period and then returning with activity. Persistent or worsening heel pain warrants a clinical review rather than a wait-and-see approach.
What are the red flags for heel pain that I should not ignore?
Seek urgent assessment if your heel pain follows a sudden injury or fall, is accompanied by significant swelling, redness, or warmth, affects both heels along with joint stiffness elsewhere in the body, or does not improve at all after six to eight weeks of conservative care. These features may suggest a fracture, infection, or inflammatory arthritis rather than straightforward plantar fasciitis, and early diagnosis makes a meaningful difference to outcomes.
What treatment options are available without surgery for bone spur vs plantar fasciitis?
Most patients with plantar fasciitis or heel spur pain do not need surgery. Effective non-surgical options include activity modification, physiotherapy and stretching programmes, supportive footwear and orthotics, anti-inflammatory medication, Coreflex Injections, Platelet-Rich Plasma (PRP) Therapy, and Peripheral Nerve Block for cases with a nerve component. The right combination depends on the underlying diagnosis, the duration of symptoms, and the patient’s overall health and activity level.
How is heel pain assessed at Singapore Paincare?
At Singapore Paincare, heel pain is assessed using the Painostic methodology, a four-pillar diagnostic framework that evaluates pain patterns, underlying pathology, pain perception, and psychological factors. Assessment includes a detailed pain history, physical examination with heel palpation and functional tests, and appropriate imaging such as X-ray or ultrasound. This multi-dimensional approach ensures the treatment plan is directed at the true source of pain rather than incidental findings on a scan.
________________________________________
About Singapore Paincare
Singapore Paincare is a specialist pain management group with clinics in Paragon and Novena. It is the first publicly listed pain management group on the Singapore Exchange (SGX). The team uses the proprietary Painostic methodology to deliver personalised, minimally invasive treatment for a wide range of acute and chronic pain conditions. No referral is needed.
Medical Disclaimer: This article is intended for general informational purposes only and does not constitute medical advice. Please consult a qualified healthcare professional for diagnosis and treatment tailored to your individual condition.